

High cholesterol isn't just a weight problem. Genetics, excess refined sugar, and thyroid dysfunction can all push your LDL into high territory, even if you're slim. Stress and poor sleep tend to affect blood lipids indirectly, through behavioral shifts rather than a direct physiological trigger. What really matters isn't the number on the scale. It's whether your LDL, HDL, and triglycerides are in balance. Together, these form your blood lipid profile, and no single number tells the whole story.
Seeing "cholesterol: borderline high" on your annual checkup is confusing, especially when you feel perfectly fine. But understanding what's actually behind it is the first step toward making a real plan.
Quick Navigation
- What Is Cholesterol — and Why Does Your Body Need It?
- Good Cholesterol vs. Bad Cholesterol — What's the Difference?
- Not Overweight — So Why Is Cholesterol Still High?
- What Should You Eat? A Practical Dietary Guide
- Natural Supplements That May Support Healthy Cholesterol Levels
- Before You Start Any Supplement — A Quick Checklist
- Developing a Cholesterol Health Product?
- FAQ
What Is Cholesterol — and Why Does Your Body Need It?
Most people hear "cholesterol" and think: cut back on fatty foods. But here's the thing — your body makes cholesterol every single day, because it genuinely can't function without it. Most of it is made by your liver; diet is just one piece of the picture. Cholesterol plays several essential roles:
- Cell membrane integrity: Every cell in your body relies on cholesterol to keep its outer membrane stable and flexible
- Hormone production: Estrogen, testosterone, and cortisol (your stress hormone) are all built from cholesterol
- Vitamin D synthesis: Your skin converts cholesterol into vitamin D when exposed to sunlight
- Bile production: Your liver uses cholesterol to make bile, which helps you digest fats
So the goal isn't to drive cholesterol as low as possible. It's to bring high LDL down to a level appropriate for your individual cardiovascular risk, while keeping HDL from dropping too low.
.png)
Good Cholesterol vs. Bad Cholesterol — What's the Difference?
A lot of people treat cholesterol and blood lipids as two separate things. They're not. Cholesterol is actually a type of blood lipid. A complete lipid panel always includes LDL, HDL, and triglycerides together.
Blood Lipids vs. Cholesterol — How Do They Relate?
Blood lipids is an umbrella term for all the fats circulating in your blood. Two main categories:
- Cholesterol: The raw material for cell structure and hormones
- Triglycerides: Your body's primary way of storing energy
Cholesterol is then further divided into LDL and HDL based on which type of "carrier protein" is transporting it:
- Blood Lipids (broad category)
- Cholesterol
- LDL (bad cholesterol)
- HDL (good cholesterol)
- Triglycerides
- Cholesterol
When you get a blood lipid panel, you'll typically see four numbers: total cholesterol, LDL, HDL, and triglycerides. That's because no single number tells the full story of your cardiovascular risk.
In everyday language, "high blood lipids" usually means something's off across the whole panel. "High cholesterol" tends to refer to elevated total cholesterol or LDL specifically. Either way, look at all four numbers together.
The Four Numbers Influence Each Other
These markers don't work in isolation. When triglycerides are high and LDL is elevated, or when HDL is low, cardiovascular risk compounds significantly, far beyond what any single number would suggest.
What Do LDL, HDL, and Triglycerides Actually Do?
Cholesterol isn't water-soluble, so it can't just float through your bloodstream on its own. It needs a carrier: a protein called a lipoprotein. Here's a simple way to think about it:
LDL is like a delivery driver. It ships cholesterol out to cells and tissues throughout your body. But when too much is delivered and it starts piling up in your artery walls, you get plaque buildup, and that's how atherosclerosis begins.
HDL is like a recycling truck. It picks up excess cholesterol from artery walls and tissues and carries it back to the liver to be processed and cleared. Low HDL is a concern, but the goal isn't to chase extremely high HDL numbers; managing LDL and overall cardiovascular risk remains the priority.
The "good" and "bad" labels for HDL and LDL are a helpful simplification. Clinically, doctors assess LDL-C alongside overall cardiovascular risk, not just the good/bad framing.
Triglycerides are a separate type of blood lipid, primarily used for energy storage. When elevated, they raise the risk of cardiovascular problems and pancreatitis.
LDL, HDL, and Triglycerides at a Glance
| Marker | Full Name | Common Name | Function | Risk When Elevated |
|---|---|---|---|---|
| LDL | Low-density lipoprotein | Bad cholesterol | Delivers cholesterol to tissues | Accumulates in artery walls; accelerates atherosclerosis |
| HDL | High-density lipoprotein | Good cholesterol | Recycles excess cholesterol to the liver | Risk applies when HDL is too LOW, not too high |
| Triglycerides | Triglycerides | Blood fats | Energy storage | Raises cardiovascular and pancreatic risk |
(Swipe left to view on mobile)
Reference Ranges (AHA / CDC Guidelines)
| Marker | Healthy Range | Borderline | Elevated / Low |
|---|---|---|---|
| Total cholesterol | < 200 mg/dL | 200–239 mg/dL | ≥ 240 mg/dL |
| LDL | < 130 mg/dL | 130–159 mg/dL | ≥ 160 mg/dL |
| HDL (male) | ≥ 40 mg/dL | 40–59 mg/dL | < 40 mg/dL (risk) |
| HDL (female) | ≥ 50 mg/dL | 50–59 mg/dL | < 50 mg/dL (risk) |
| Triglycerides | < 150 mg/dL | 150–199 mg/dL | ≥ 200 mg/dL |
(Swipe left to view on mobile)
Source: AHA; CDC. Note: the AHA uses more granular LDL categories (e.g., < 100 mg/dL as "optimal"). The ranges above reflect general screening thresholds. Individual treatment targets should be set by your doctor based on age, diabetes status, cardiovascular history, and other personal risk factors.
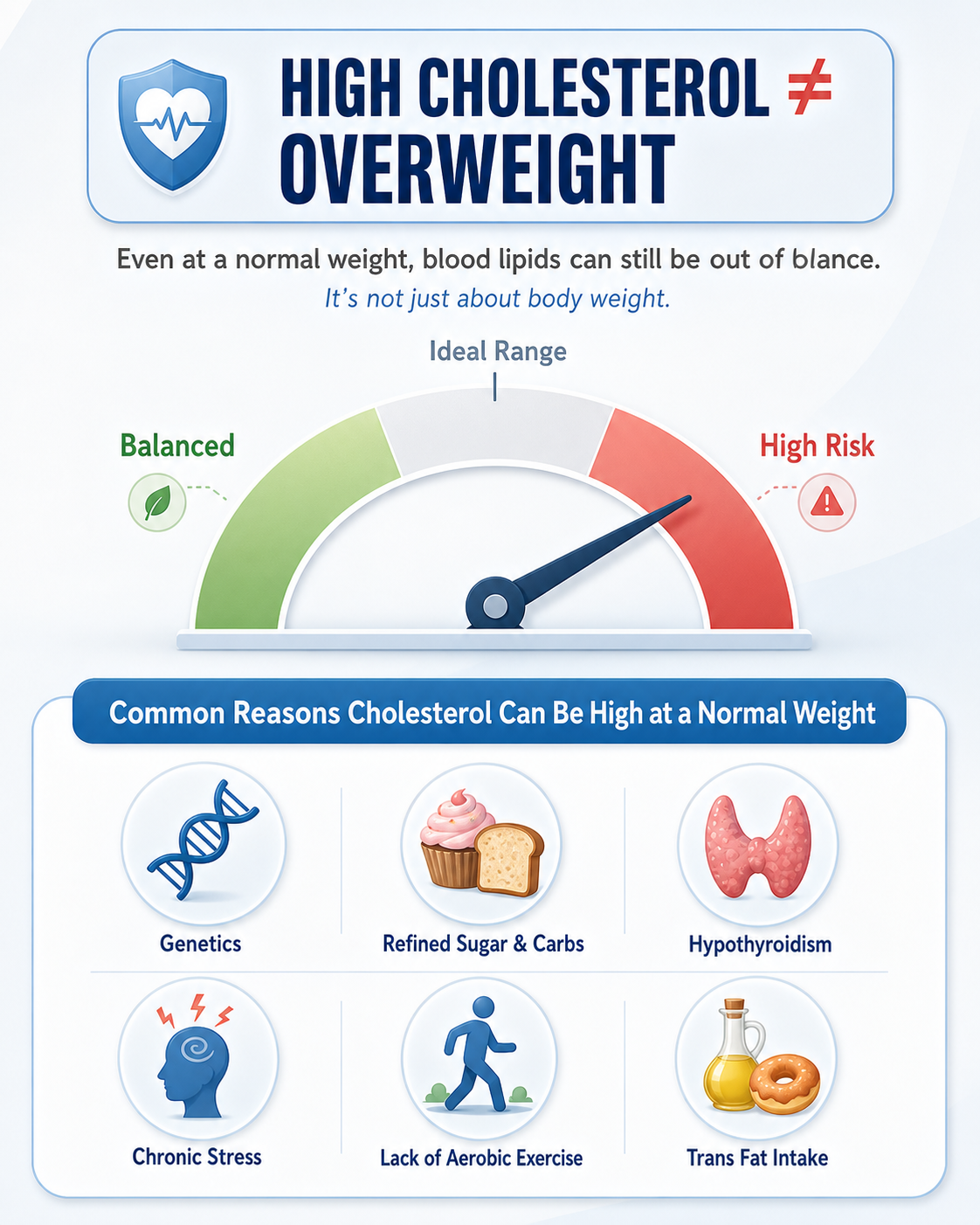
Not Overweight — So Why Is Cholesterol Still High?
Weight gets blamed a lot. But it's just one of many contributing factors. Here are the ones that most often go overlooked:
1. Genetics — Familial Hypercholesterolemia (FH)
Think of your liver as having a row of recycling bins (LDL receptors) that pull LDL out of the bloodstream and break it down. In people with Familial Hypercholesterolemia (FH), those bins are defective from birth — no matter what they eat or how slim they are, LDL simply doesn't get cleared properly. The problem is genetic, not dietary. Studies suggest FH affects roughly 1 in 250–311 people worldwide, depending on the population and diagnostic criteria. It's one of the most common — and most underdiagnosed — genetic causes of high LDL in people who aren't overweight.
Source: CDC | About Familial Hypercholesterolemia
2. Too Much Refined Sugar and Refined Carbohydrates
The more typical effect of excess sugar and refined carbs is elevated triglycerides and lower HDL, not necessarily higher LDL. Your liver is remarkably efficient: when more sugar comes in than your body can use, it converts the excess into fat, raising triglycerides in the process. If lowering LDL is the primary goal, saturated fat and trans fat are the more direct culprits.
3. Chronic Stress and Lifestyle Patterns
Stress genuinely affects blood lipids, but the pathway is more indirect than most people realize. It's not a straight line from "stress → cholesterol spike." What happens is a cascade: poor sleep, disrupted eating, more alcohol, and less movement, all feeding into each other. That's why some people notice their numbers quietly rising during the busiest periods of their careers.
4. Hypothyroidism
Thyroid hormones act like an efficiency manager for your liver's LDL recycling process. When thyroid function drops, LDL receptor numbers decrease and clearance slows, meaning LDL stays in the bloodstream longer, even with a clean diet. This is especially common in middle-aged women and often gets mistaken for a dietary issue. When LDL is notably elevated, ruling out thyroid dysfunction is a worthwhile step.
5. Not Moving Enough? It Shows Up in Your Numbers
Regular aerobic exercise has consistent positive effects on blood lipids, particularly for triglycerides and HDL. AHA data shows that increased physical activity can raise HDL by roughly 1–2 mg/dL and lower triglycerides by 4–12 mg/dL. For meaningful LDL reduction, exercise alone usually isn't enough; it works best alongside dietary changes and weight management.
6. Trans Fat Intake
Even in people at a healthy weight, long-term consumption of trans fats — found in partially hydrogenated vegetable oils — raises LDL and lowers HDL simultaneously. They're the worst type of dietary fat for your heart. See WHO Trans Fat Fact Sheet.
When Numbers Jump Suddenly — Check for Secondary Causes
If your diet hasn't changed much but a recent checkup shows LDL or triglycerides significantly higher than before, a doctor will typically rule out secondary causes first:
- Hypothyroidism (most common)
- Diabetes or poor blood sugar control
- Medication side effects (e.g., corticosteroids, certain diuretics, estrogen)
- Kidney disease (nephrotic syndrome) or liver conditions (cholestatic liver disease)
- Heavy alcohol use
This step matters. When a secondary cause is driving the change, diet adjustments alone rarely move the numbers. Knowing whether you're dealing with a lifestyle issue or an underlying medical condition is what points you toward the right fix.

What Should You Eat? A Practical Dietary Guide
Foods to Prioritize
| Food Type | Examples | How It Helps |
|---|---|---|
| Soluble dietary fiber | Oats, barley, legumes, apples, psyllium | Binds bile acids; promotes cholesterol excretion |
| Healthy fats | Olive oil, avocado, nuts | Replacing saturated fats with unsaturated fats helps improve LDL-C and overall cardiovascular health |
| Fatty fish | Salmon, mackerel, sardines | Rich in omega-3s; helps lower triglycerides |
| Soy and legumes | Edamame, tofu, soy milk | Soy protein may offer a modest LDL-lowering effect (around 3–4%) |
| Vegetables and whole foods | Spinach, broccoli, legumes | More whole plant foods support overall cardiovascular health |
(Swipe left to view on mobile)
Foods to Limit or Avoid
| Food Type | Examples | Effect |
|---|---|---|
| Trans fats | Some crackers, flaky pastry, non-dairy creamer | Raises LDL and lowers HDL simultaneously |
| Refined sugar and sweetened drinks | Sugary beverages, desserts, white sugar | Elevates triglycerides |
| Processed meats | Sausage, bacon, hot dogs | High in saturated fat and sodium |
| Excess saturated fat | Fatty meats, full-fat dairy (moderate amounts are fine) | Too much will raise LDL-C |
(Swipe left to view on mobile)
The bigger picture: The Mediterranean diet is consistently backed by research and AHA guidelines as one of the most heart-protective dietary approaches available. The PREDIMED trial (7,447 high-risk adults; findings confirmed after re-analysis) showed that a Mediterranean-style diet with extra-virgin olive oil or nuts reduced major cardiovascular events by around 30%. That effect comes from the overall eating pattern; no single ingredient gets the credit.
Eating Out? Start with These Ground Rules
Getting the theory right is one thing. Sticking to it when eating out is another. Perfection isn't the goal, but a few bottom-line rules go a long way:
- Keep fried food to no more than once a week
- Cut sugary drinks from daily to no more than once a week; go unsweetened the rest of the time
- Default to grilled, braised, or steamed for main dishes over fried
- Add a serving of fiber (oats, legumes, vegetables) to every meal
Starting with these two categories — fried food and sugary drinks — tends to produce the most noticeable shift in blood lipids without requiring a complete dietary overhaul.
A Practical Dining Guide for Eating Out
| Setting | Better Choices | What to Skip | Why It Matters |
|---|---|---|---|
| Fast food | Grilled chicken sandwich + side salad + water or unsweetened iced tea | Double cheeseburger, large fries, milkshake combo | A typical combo can pack 30–40g of saturated fat, close to two days' worth |
| Coffee shop | Black coffee or unsweetened latte + oatmeal or a whole grain item | Flavored syrup drinks, whipped cream lattes, butter croissants | Specialty drinks can easily add 40–60g of sugar before 9 a.m., directly pushing triglycerides up |
| Casual diner | Grilled or baked fish or chicken + vegetables + whole grain side | Creamy pasta, fried appetizers, thick gravy dishes | Saturated fat hides in sauces and cooking methods; grilled or baked always wins |
| Pizza | Thin crust + vegetable toppings, 1–2 slices | Deep dish, stuffed crust, pepperoni or sausage heavy | Processed meat toppings are among the most saturated-fat-dense items in a typical restaurant meal |
| Bar food / late night | Baked or grilled options, hummus and vegetables, unsweetened drink | Fried wings, loaded nachos, sugary cocktails | Fried bar food is often the highest-saturated-fat meal of the week; managing how often you go matters more than finding the perfect swap |
| Deli / work lunch | Turkey or chicken on whole grain + plenty of vegetables, mustard over mayo | Pastrami or salami subs, extra cheese, heavy condiments | Processed deli meats are high in sodium and saturated fat even before you add sides |
| Smoothie / juice bar | Whole-fruit blend with protein, no added sugar | "Detox" juice blends, sugar-added acai bowls, cream-based smoothies | Liquid sugar raises triglycerides just as effectively as solid sugar, and goes down much faster |
(Swipe left to view on mobile)
Natural Supplements That May Support Healthy Cholesterol Levels
When diet alone isn't enough — or genetics are a factor — the following supplements have scientific evidence behind them. One important note first: supplements play a supporting role. They shouldn't replace dietary changes, regular exercise, or medical evaluation when needed. In terms of evidence strength, soluble fiber and plant sterols have the most robust research for LDL reduction; omega-3s are most relevant for high triglycerides; red yeast rice carries significant safety considerations; and curcumin and CoQ10 are best positioned as secondary support.
1. Soluble Dietary Fiber (as a Supplement)
If hitting your daily fiber goals through food alone is a challenge, soluble fiber — like oat beta-glucan or psyllium — is one of the most evidence-backed supplemental options for blood lipids. A 2023 dose-response meta-analysis covering 181 RCTs and 14,505 participants found that soluble fiber modestly reduced LDL-C, total cholesterol, and triglycerides. Adding 5g per day was associated with an additional ~5.57 mg/dL drop in LDL. That said, fiber supplements work best alongside broader dietary changes — not as a standalone fix.
2. Plant Sterols / Phytosterols
Plant sterols look similar enough to cholesterol that they compete for the same absorption sites in the intestine, crowding out dietary cholesterol before it enters the bloodstream. Studies show that around 2g per day typically lowers LDL-C by 5–15%. A few caveats worth knowing: these products can't replace prescription medications, and no large randomized trial has yet directly shown they reduce heart attacks or strokes. People with a rare metabolic condition called sitosterolemia should avoid them entirely.
Sources: NHLBI TLC Guide; Nutrition Reviews Plant Sterol Umbrella Review
3. Omega-3 Fatty Acids (EPA / DHA)
The clearest benefit of omega-3s is lowering triglycerides, not LDL. Keep in mind that everyday fish oil supplements and prescription omega-3 products differ significantly in concentration, dose, and evidence base. The AHA cites prescription-grade omega-3 at around 4g/day, which can lower triglycerides by 20–30% in most people. If your triglycerides aren't elevated, using omega-3 as a primary LDL-lowering strategy is unlikely to work well, and in some people, DHA-based formulas may cause a modest LDL increase. If you're taking anticoagulant medications, consult a healthcare provider before starting.
→ Further reading: Omega-3 Benefits, Sources, and Foods | What Is Algae Oil?
4. Red Yeast Rice (Monacolin K)
Monacolin K — the active compound in red yeast rice — is chemically identical to lovastatin, a prescription statin. Products with sufficient monacolin K content can lower LDL-C, but that also means the same side effect profile applies: muscle discomfort, elevated liver enzymes, drug interactions, and variable product quality (including the risk of citrinin contamination).
Important regulatory update (2024): The European Commission withdrew the health claim for red yeast rice and restricted its use in food supplements containing ≥ 3 mg/day of monacolins, citing safety concerns. NCCIH also clearly states that red yeast rice containing monacolin K should be treated with the same caution as lovastatin.
If you have a history of liver disease or muscle problems, are currently taking statin medications, or are pregnant or breastfeeding, talk to your doctor before using these products.
5. Curcumin
Curcumin has antioxidant and anti-inflammatory properties. A 2025 updated umbrella review — covering 26 systematic reviews and meta-analyses across roughly 4,630 participants — found an average LDL-C reduction of about 5.84 mg/dL, with modest improvements in triglycerides and total cholesterol. That said, study heterogeneity is high, and the evidence quality for LDL was rated "very low." It's best positioned as a possible supporting ingredient. Low bioavailability is an ongoing challenge; enhanced delivery formats like micronized or liposomal curcumin may improve uptake.
6. CoQ10 — Worth Considering if You're on Statins
Statins suppress CoQ10 production as a side effect, since both share the same biosynthetic pathway. Some small studies and recent reviews suggest CoQ10 supplementation may help with statin-associated muscle symptoms, but findings are inconsistent. CoQ10 is not a cholesterol-lowering agent. If muscle discomfort appears after starting statin therapy, talk to your doctor to rule out other causes before deciding whether to supplement.
Before You Start Any Supplement — A Quick Checklist
- Red yeast rice + cholesterol medication: Talk to your doctor first to confirm whether combining them is appropriate
- Omega-3 (standard doses): Generally safe, but if you're taking more than 3g/day or are on anticoagulants, check with your doctor first
- Severely elevated levels: LDL ≥ 190 mg/dL or triglycerides ≥ 500 mg/dL, especially alongside other cardiovascular risk factors: get a medical evaluation. Supplements support treatment; they don't replace it
- Give it time: Dietary and supplement changes take time to show up in lab work. Recheck your blood lipids after about 3 months to see where things are heading
Developing a Cholesterol Health Product?
Each ingredient covered above — soluble fiber, plant sterols, omega-3, and red yeast rice — comes with its own formulation and regulatory considerations. Boncha Bio provides nutraceutical ODM services, with an existing chewable granule lineup that includes fish oil, algae oil, and turmeric as a starting point. If you have a product concept in mind, contact us and we're happy to explore the right development path together.
FAQ
Q1: Why would a slim person have high cholesterol?
A: Cholesterol levels are driven more by genetics, diet quality (especially refined sugar and saturated fat), and thyroid function than by body weight. Stress and poor sleep tend to influence blood lipids through indirect behavioral pathways. Familial hypercholesterolemia is the most common genetic cause of high LDL in people who aren't overweight — even with an entirely clean diet, LDL can remain elevated.
Q2: What LDL level is considered high?
A: General screening guidelines (AHA / CDC) classify LDL < 130 mg/dL as acceptable for most people; 130–159 mg/dL is borderline high, and ≥ 160 mg/dL is elevated (see the reference table in this article). Treatment targets vary based on individual cardiovascular risk; blood pressure, blood sugar, and smoking history all factor in. Elevated numbers don't automatically mean medication is needed; that's a decision for you and your doctor.
Q3: Can omega-3 lower cholesterol?
A: Omega-3s (EPA/DHA) work primarily on triglycerides, not LDL. If your triglycerides aren't elevated, using omega-3 to target LDL is unlikely to be effective, and in some people, standard fish oil may cause a modest LDL increase. Also worth noting: OTC fish oil and prescription-grade omega-3s are not interchangeable in terms of concentration or clinical evidence.
Q4: Can you take red yeast rice and cholesterol medication together?
A: Both work through the same mechanism, so combining them can produce additive effects. Let your doctor know about your current medications before starting, and have them assess whether any adjustment is needed.
Q5: How often should you get blood lipids tested?
A: For generally healthy adults, the CDC recommends a baseline test starting at age 20, then every 4–6 years if results are normal. If your numbers are elevated, you've recently made significant lifestyle changes, or you've started medication, retesting after 8–12 weeks to 3 months is a reasonable way to track progress. Your doctor may recommend more frequent monitoring depending on your overall cardiovascular risk profile.
Conclusion
High cholesterol isn't just a problem for people who are overweight. Genetics, dietary patterns, thyroid function, and lifestyle habits all play a role. Understanding the LDL/HDL distinction and knowing which factors are actually driving your numbers is the difference between wishful thinking and a plan that works.
Building from a solid dietary foundation — more soluble fiber, healthier fat choices, less refined sugar and trans fat — is the most evidence-backed place to start. Regular exercise delivers consistent benefits for triglycerides and HDL. For additional support, soluble fiber supplements, plant sterols, and omega-3s each have a reasonable evidence base; red yeast rice can be effective but carries safety considerations that make a conversation with your doctor worthwhile first.
Boncha Bio can support every stage of product development — from ingredient evaluation and formulation design to regulatory documentation — across a range of markets. Our current chewable granule direction includes fish oil, algae oil, and turmeric. Whether a specific health claim is approvable will depend on the applicable regulations and final submission results. If you have a concept in mind, contact us to explore the path forward.
Medical Disclaimer
The content in this article is for general health and nutrition education only. It is not a substitute for medical diagnosis or treatment advice. If your LDL-C is significantly elevated (e.g., ≥ 190 mg/dL), triglycerides are very high (e.g., ≥ 500 mg/dL), you have a family history of early-onset cardiovascular disease, or you have diabetes, thyroid dysfunction, kidney disease, liver disease, or similar conditions, please consult a healthcare professional for individualized evaluation and a treatment plan.
References
Blood Lipid Basics and Health Education
- Taiwan NHA | Is Dyslipidemia Always About High Cholesterol?
- Taiwan NHA | Adult Preventive Health Services
- CDC | About Cholesterol
- CDC | LDL, HDL Cholesterol and Triglycerides
- CDC | Cholesterol Myths and Facts
- CDC | Testing for Cholesterol
- AHA | Cholesterol Overview
Causes and Mechanisms
- CDC | About Familial Hypercholesterolemia
- PubMed 22717171 | Impact of Stress Systems and Lifestyle on Dyslipidemia
- NCBI Endotext | Hypothyroidism and Lipid Metabolism
- PMC 3109527 | Effects of Thyroid Dysfunction on Lipid Profile
- AHA | Physical Activity as a Critical Component for Elevated Cholesterol
- WHO | Trans Fat Fact Sheet
- NCBI Endotext | Secondary Dyslipidemia
Diet and Supplements
- AHA | Diet and Lifestyle Recommendations
- AHA | Mediterranean Diet
- Harvard T.H. Chan School of Public Health | PREDIMED Re-analysis Explained
- AHA Journals | Guideline on the Management of Blood Cholesterol
- AHA | Saturated Fats
- ScienceDirect 2023 | Soluble Fiber Dose-Response Meta-Analysis on LDL-C
- NHLBI | Your Guide to Lowering Your Cholesterol With TLC
- Nutrition Reviews | Plant Sterols Umbrella Review
- AHA | Prescription Omega-3 Medications Work for High Triglycerides
- NCCIH | Omega-3 Supplements: What You Need to Know
- NCCIH | Things to Know About Omega-3s for Heart Disease
- NCCIH | High Cholesterol and Natural Products
- PMC 5637251 | Efficacy and Safety of Turmeric and Curcumin in Lowering Blood Lipid Levels
- PubMed 37856800 | Curcumin Updated Umbrella Review 2025
- PubMed 31006811 | Soy Protein and LDL Reduction
- PMC 12554813 | Related Study
Regulatory
- Taiwan TFDA | Guidelines on Food Advertising Claims
- Taiwan TFDA | Red Yeast Rice Health Food Standards
- EU Commission Regulation (EU) 2024/2041 | Red Yeast Rice Health Claim Withdrawal
.jpg)